What leaner ICBs mean for outcome measurement in the NHS
ICBs are halving running costs and becoming strategic commissioners; the organisations that build a consistent, credible way of evidencing outcomes now will be better placed to commission well within their new constraints.
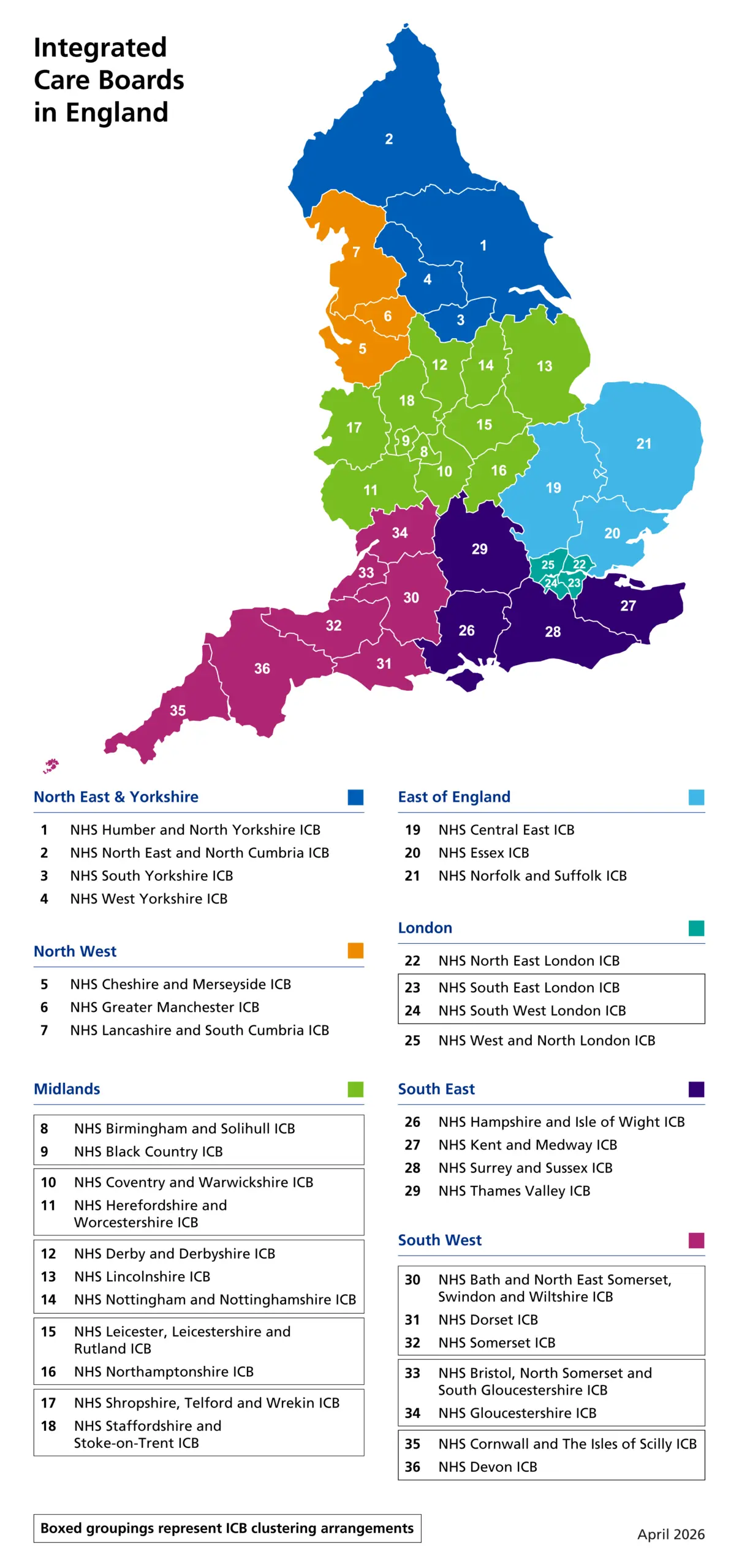
The reorganisation of England's integrated care boards has moved quickly. In March 2025 NHS England told ICBs to cut their running costs by half, and over the following year most agreed clustering arrangements to operate across larger footprints. On 1 April 2026 the first wave of formal change took effect, with twelve ICBs abolished and six new ones established, and further boundary changes are scheduled for April 2027 as ICBs move towards sharing borders with strategic authorities. The forty-two boards that existed two years ago are consolidating into a smaller number of larger organisations operating within a tighter running cost cap.
Most of the coverage has focused on what this means for jobs and structures, which is understandable given the scale of the redundancies involved. The quieter shift is in what ICBs are now expected to do. The role has been narrowed to that of strategic commissioner: an organisation whose job is to purchase care that moves resource out of hospitals and into communities, rather than to manage local systems in the round. That is a change in purpose, not only in size.
The questions a strategic commissioner has to answer
A strategic commissioner buying for outcomes needs to know two things that a system manager could afford to treat as secondary. The first is whether the things being commissioned are actually what the local population needs. The second is whether the money spent produced the change it was meant to produce. Both are measurement questions, and both become harder to answer credibly when the teams who used to hold that knowledge are smaller.
This is the tension at the centre of the reorganisation. ICBs are being asked to commission more deliberately at the same time as they lose capacity to evidence their decisions. The instinct under financial pressure is to track what is easy to count: the number of services procured, the volume of activity delivered, the contractual commitments made by suppliers. Those figures are necessary for assurance, but they describe what was bought rather than what changed for residents. The distinction matters more for a strategic commissioner than it did for a system manager, because the strategic commissioner is being judged on whether resource genuinely shifted towards prevention and community care. This is the difference between measuring outputs and measuring outcomes, and it sits at the centre of how we think about the Public Outcomes Lifecycle.
The policy environment is pulling the same way
The policy environment is pulling in the same direction. The NHS Social Value Playbook asks NHS buyers to apply a minimum social value weighting across procurement and ties social value to health inequalities through Core20PLUS5. The Local Outcomes Framework published by MHCLG in February 2026 sets out priority outcomes for local government drawn from official statistics, and the relationship between ICBs, councils and combined authorities is becoming more closely aligned as ICB boundaries move towards coterminosity with strategic authorities. The direction of travel across health and local government is towards outcomes, place and the wider determinants of health. The structures are being reshaped to commission against that direction, but the measurement practice has to catch up with it.
Evidencing outcomes with less capacity
For commissioners working through this, the practical question is how to evidence outcomes without rebuilding the analytical capacity that has just been cut. That is where established methodology earns its place. Social Return on Investment and theory of change are not new techniques, and the value of using them is precisely that they do not need to be reinvented for each ICB. A consistent way of valuing outcomes, applied across a portfolio of commissioned services, lets a leaner organisation produce credible evidence without a large in-house analytical team. This is what the platform is built to do, drawing on an established proxy library so that valuation rests on a shared basis rather than case-by-case judgement. Where an ICB needs that methodology signed off by an accredited practitioner, Social Value Direct provides the assurance layer.
Consistency also makes aggregation possible. A strategic commissioner with a wider footprint needs to compare and combine impact across the services it buys, which is difficult when each one is measured differently. Understanding the population being commissioned for is the starting point, and tools such as Place Explorer exist to profile local need so that commissioning decisions begin from evidence about the place rather than assumption. You can read more about Place Explorer and the wider platform on our about page.
If you want to test the financial case for a commissioned service quickly, the SROI Calculator provides an accessible starting point for commissioners and providers working through an initial estimate before a full appraisal.
Where this leaves ICBs
None of this makes the reorganisation easier in the short term. The immediate task for most ICBs is to stabilise within their new running cost cap, and measurement will not be the first thing on the list. But the role they are being moved into is one where the ability to show what their spending changed is no longer a reporting nicety. It is the basis on which a strategic commissioner makes its case. The organisations that come through the reorganisation with a clear, consistent way of evidencing outcomes will be better placed to commission well within their new constraints than those that fall back on counting activity.
The Social Value Engine works with commissioners and funders on exactly this question, including NHS bodies such as Lincolnshire Partnership NHS Foundation Trust. If you would like to talk about measuring the outcomes of what you commission, you can find more on our NHS and social care page or read about our approach on the about page. You are also welcome to get in touch directly.
Frequently asked questions
Expand a question to read the answer.
An integrated care board (ICB) is an NHS organisation responsible for planning and buying health services for a defined area of England. Following the 2026 reorganisation, ICBs have been consolidated into a smaller number of larger bodies with a tighter running cost cap, and their role has been narrowed to that of strategic commissioner — purchasing care that moves resource from hospitals into communities.
Stay informed
Get insights on social value delivered to your inbox